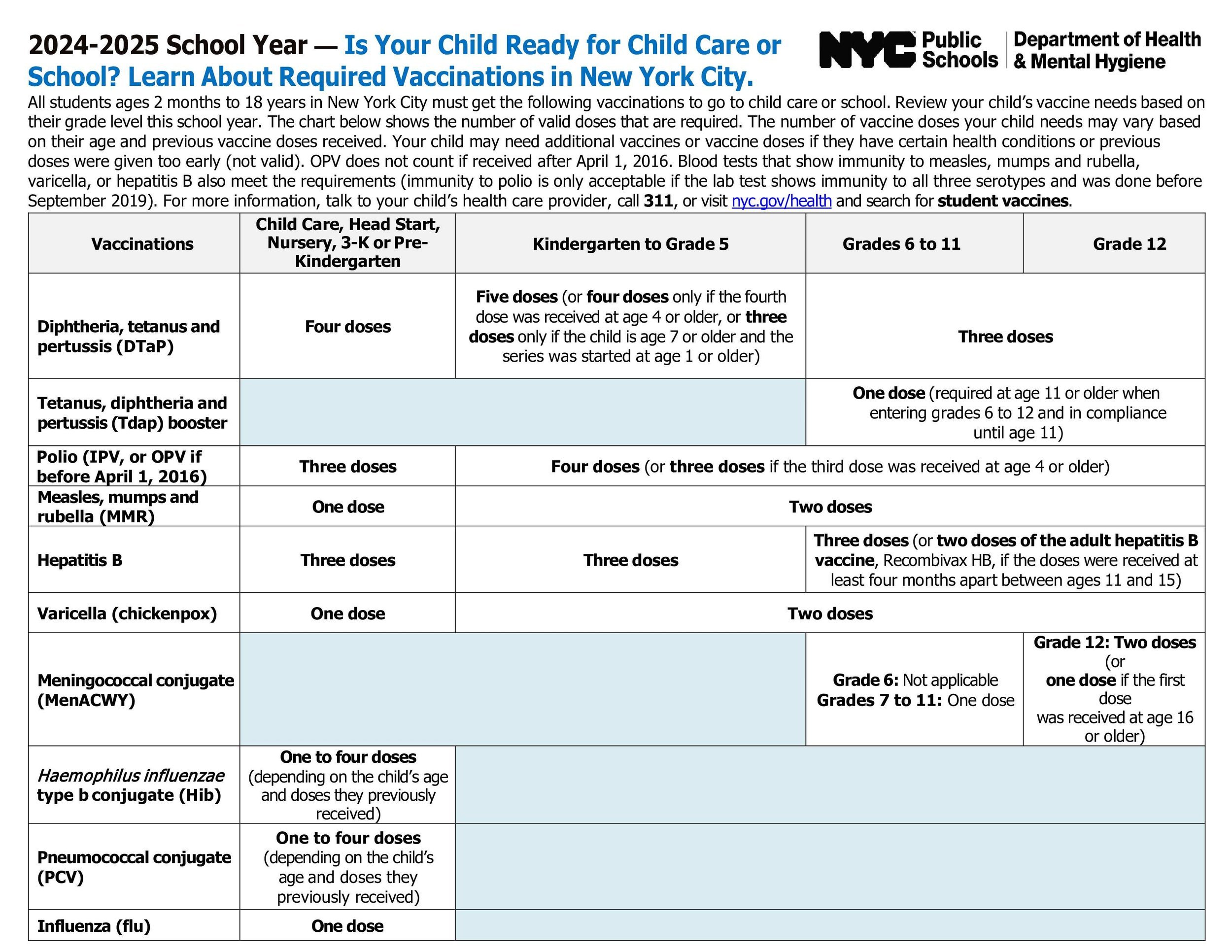
Please submit the form below before the start of the program (filled out, signed and stamped by the pediatrician’s office).
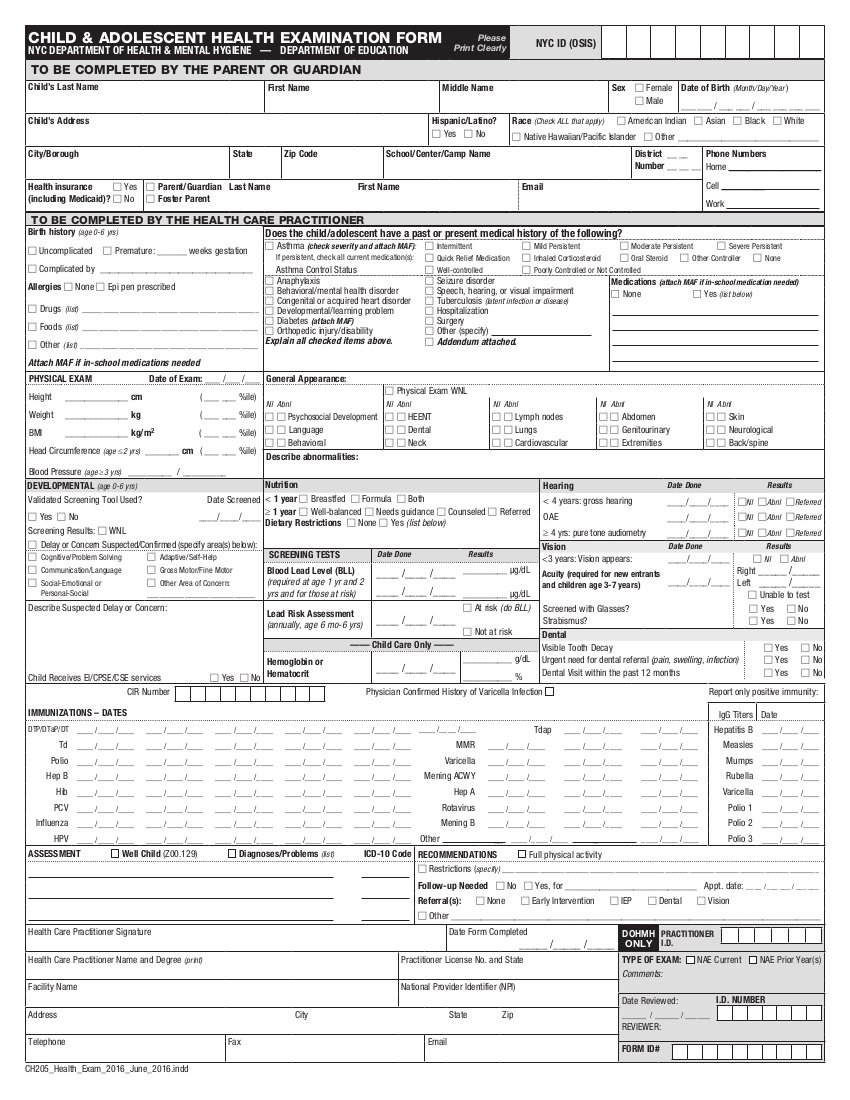































________________________________________________________________________________________________________________________
Pictures from previous years below - Summer Recreational Program.